by Jan Hach, MD
From the very beginning, the use of artificial joint replacements has been accompanied by greater or lesser problems of wear or even spontaneous degradation of materials from which the endoprostheses are made. Nowadays, polyethylene disease is well known as is ARMD (Adverse Reaction to Metal Debris) arising around MoM (metal-on-metal) type endoprostheses. Metal wear is problematic because it releases toxic chromium and cobalt ions into the body.
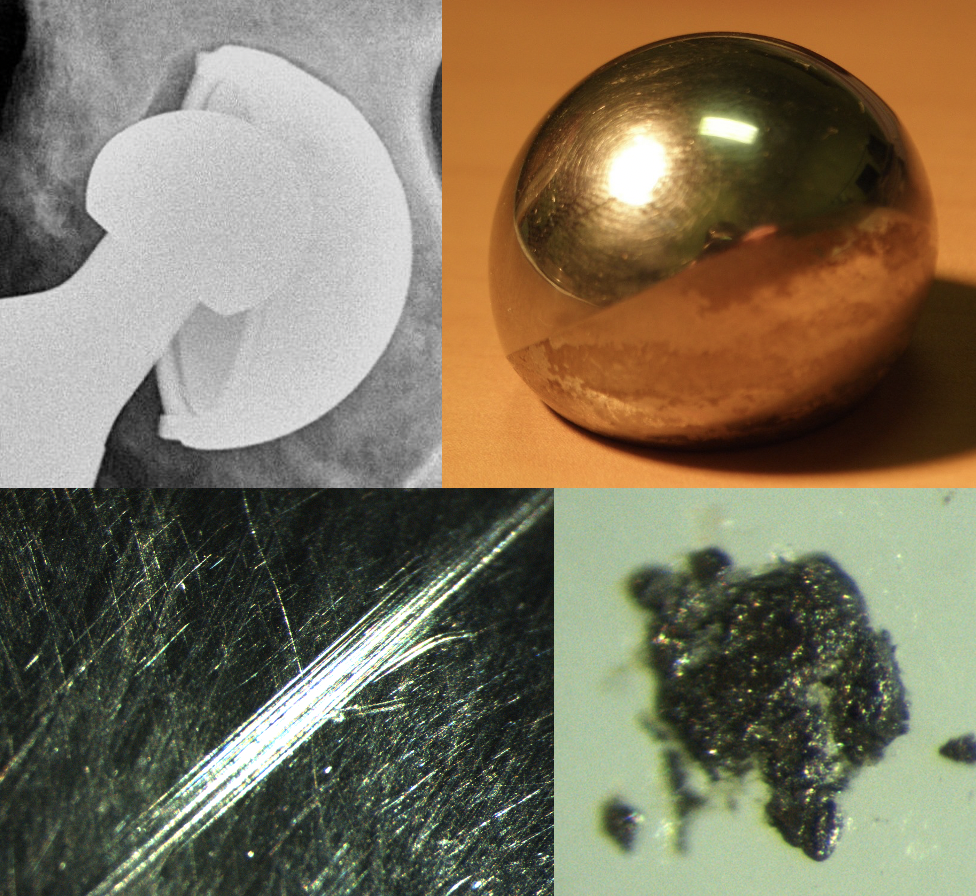
Damaged Femoral Head Component
The above images represent a failed acetabular component with damage to the femoral head including scratches on the surface and micro-debris.
Metal wear can occur for reasons other than just MoM wear. It has to do with which materials are harder than cobalt-chromium alloy. The main one is ceramics. Next is titanium which is roughly the same on the hardness scale as Co-Cr (cobalt-chromium alloy). Are you aware of the effect of different types of bone cement? Methyl methacrylate is a relatively soft substance itself, but it usually contains radiopaque additives. Due to the additives used, we classify cements as “soft” or “hard”. Cement producers use either barium sulphate (softer than steel and CoCr) or zirconium, which is harder than them. Incidentally, bone minerals such as tricalcium phosphate and hydroxyapatite) are slightly softer than Co-Cr.
In recent years we have learned to not use Co-Cr heads in hip revision operations that were required by destruction of a ceramic articulating component. Even small amounts of ceramic particles embedded in the socket can cause a metal head to rapidly abrade. In my experience, the same problem can occur as a result of the presence of particles from “hard” bone cement and titanium resulting from surgery on the other components. Therefore, I recommend using revision ceramic heads with titanium sleeves (taper adaptor) for all revision procedures. The only exception is when I am sure of the composition of the bone cement used in the primary operation and the material from which the previously used components were made.
Dr. Hach practiced for 15 years with the professors who began joint replacement in the Czech Republic in the 1960s and 1970s where he taught medical students as an assistant professor. Currently he is Chair of the Orthopedic Department in Melnik, Czech Republic. In addition, since 2002 he has been the Implant Database Manager on the team that manages the National Registry of Joint Replacement.